- Research
- Open access
- Published:
Unveiling health disparities in Palestine: a qualitative study of stakeholders' perspectives
International Journal for Equity in Health volume 24, Article number: 102 (2025)
Abstract
Background
Healthcare services in Palestine are provided by the Ministry of Health, the United Nations Relief and Works Agency, Non-Governmental Organizations and private sector. These providers have played a complementary role in improving health services and the overall health situation in Palestine over the past two decades. However, health disparities in Palestine remain numerous; several health reports and surveys have indicated significant disparities in health outcomes within the Palestinian community. The Palestinian political, social, and economic contexts contribute to increased risk of health inequities in various aspects. This study explored these disparities in the healthcare from the perspectives of key sectoral stakeholders.
Methods
The study adopted a qualitative design to explore the perspectives of key stakeholders regarding health disparities within the Palestinian healthcare system. Sixteen in-depth interviews with purposefully selected key informants were carried out. We conducted content analysis to extract emerging themes and subthemes.
Results
Three main themes and eleven subthemes were realized from participants’ perceptions. The major three themes are: areas of health disparities, contributing factors to health disparities, and policy recommendations to enhance health equity. Three subthemes were recognized as main areas of health disparities: (1) healthcare services’ provision, (2) health coverage and (3) health outcomes. Three subthemes were recognized as main contributing factors that are: (1) political factors, (2) socioeconomic and cultural factors, and (3) health system factors. Five main subthemes were recognized as major policy recommendations suggested by participants to enhance health equity: (1) Integrating health equity into policy frameworks, (2) Strengthening MoH leadership and fostering collaborative partnerships to advance health equity, (3) Enhancing healthcare infrastructure and delivery approach (4) Reforming the health insurance system for better equity and efficiency and universal coverage, and (5) Fostering community awareness and advocacy for advancing health equity and the right to health for all Palestinians.
Conclusion
This study identified significant policy debates about health disparities and its contributing factors in Palestine, arguing to drive evidence-based policy making and comprehensive reforms in the Palestinian health system to improve equity in healthcare access and coverage.
Introduction
Addressing health inequities has been a longstanding global concern in the efforts to achieve social justice for all. The worldwide 2030 commitment of leaving no one behind has prioritized addressing disparities, including health disparities, as a key focus of national and global policy agendas.
Health equity is considered a moral and ethical principle; health inequities are considered unfair avoidable disparities [1]. Health equity is also conjugated with the human rights theme of health; “equity in health implies that ideally everyone could attain their full health potential and that no one should be disadvantaged from achieving this potential because of their social position or other socially determined circumstance” [2]. Achieving health equity involves reducing and ultimately eliminating disparities in health and its determinants that adversely affect marginalized groups [3].
Health disparities in Palestine are numerous; several health reports and surveys have indicated disparities in health outcomes within Palestinian community [4]. These disparities were primarily associated with the Israeli occupation and its political implications, which are usually described as barriers to healthcare access [5,6,7]. The lack of adequate disaggregated data for many health indicators by geographical location limits the analysis of health inequities [8]. Moreover, the Palestinian political, social and economic contexts contribute to an increased risk of health inequities in various aspects.
Studying and tackling health disparities is a core issue to support national efforts towards achieving universal health coverage and sustainable development in health. It also contributes to prioritizing health equity on the national policy agenda. This study seeks to draw attention to the critical need for developing and implementing effective interventions aimed at identifying and addressing health disparities in Palestine.
The Palestinian context
The 5.48 million Palestinian population has unique demographic, social and political characteristics that significantly impact their health status. The Palestinian community is notably young, with 47.6% of the population is under 19 years old and relatively high fertility rates. About 78% of the population lives in urban areas, 14% in rural areas and 8% in overcrowded refugee camps. Very high population density is noticeable specially in Gaza Strip that reached up to 6,102 persons/ km2 in Gaza Strip in mid-2023 [9]. These discrepancies in living conditions contribute to health disparities, affecting access to healthcare, sanitation, and healthy living environments.
Education is a crucial social determinant of health, influencing employment opportunities, health literacy, and access to health resources. The Palestinian community is characterized by high education rates for both males and females, but still women participation in labour force remains relatively low. While the illiteracy rate among adults reached 2.2% [9], women’s participation in the labour force reached only 19% of the total number of women of working age in 2022 [9]. The unemployment rate among the youth graduates (19–29 years) reached 48%, with a significant gender disparity (61% among females compared to 34% for males) [9].
The Palestinian political landscape marked by the ongoing Israeli occupation has imposed substantial restrictions on movement between Palestinian cities and villages, Israeli checkpoints and closure of Palestinian cities have further fragmented the Palestinian territories into small enclaves. These restrictions have created a significant socioeconomic disparity between the West Bank and the Gaza Strip, with poverty levels more heavily concentrated in Gaza. The division of the West Bank under the Oslo Accords, into East Jerusalem and Areas A, B and C, each is governed by different security regulations, has further complicated access to health care, education, livelihoods, and economic opportunities [10]. In 2022, Poverty affected 24.3% of Palestinians, with unemployment rate at 24.7% across Palestine and 46.4% in Gaza Strip [10].
Palestinian health system
The Palestinian health sector consists of four main health service providers: Palestinian Ministry of Health (PMoH), the United Nations Relief and Works Agency (UNRWA), Non-governmental organizations (NGOs) and private sector. These sectors played a complementary role in improving health services and the health situation in Palestine over the past decade. The public sector makes up the bulk of the health service delivery system in Palestine through a network of governmental primary health care centers and governmental hospitals in the different governorates. UNRWA is the second main provider of primary healthcare services in Palestine after PMoH, targeting Palestinian refugees who live in overcrowded camps under poor living conditions and inadequate sanitation and hygiene services.
Four main schemes of health insurance are available in Palestine, that are the Governmental Health Insurance system, UNRWA health insurance scheme that covers Palestinian refugees, Military Services Health Insurance and Private health insurance. According to PCBS Census of 2017, 79% of population is covered by at least one type of health insurance scheme, and about 20% of the Palestinian population are not covered by any type of health insurance [11].
The Governmental Health Insurance scheme is considered the main scheme in the Palestinian community as it has the highest coverage in terms of population and services. It was issued in the year 2004 and offers obligatory enrolment for public sector employees and voluntary enrolment for any Palestinian citizen. The current governmental health insurance scheme is considered a very generous scheme as it offers high coverage for a wide range of services, but also has been criticized for its poor equity and efficiency [12]; any sick person can join the insurance system and immediately access the same benefits as healthy individuals who have been contributing for the system for long years. From an efficiency perspective, the system revenues are considered very minor compared to total PMoH expenditure [12, 13].
The Palestinian humanitarian and health conditions are fragile; access to healthcare services in Palestine is negatively affected by several issues including Israeli occupation policies, financial obstacles, lack of specialized care and qualified specialized doctors. In addition to increasing rates of non-communicable diseases and increasing health demands [14]. The implementation of a complex permit regime, as well as the expansion of settlements and the movement restrictions in Area C, constrain movement within and across the Palestinian cities and villages. More than two million Palestinians living in Gaza Strip have been suffering under complete blockade since 2007. The political division between the West Bank and Gaza further complicates coordination in the delivery of essential health services [10].
From another perspective, the various challenges facing the governmental health sector have negatively affected the quality of care provided by public services, resulting in long waiting times, overwhelmed staff due to high workload and lack of incentives, shortages in essential medicines and laboratory materials, old and poor infrastructure in many public hospitals [15, 16].
Understanding health disparities and why they exist involves identifying factors that explain gaps in healthcare services or health outcomes between different community groups. Studying potential factors or determinants that might explain the existence of health disparities would inform policies or interventions to reduce or eliminate these differences. This study aims to explore the perspectives of key stakeholders about the current health disparities within the Palestinian health system. Specifically, it seeks to understand their perception regarding the key areas of inequity, and the underlying causes of these inequities. Additionally, the study examines stakeholders' views on the findings of the 2019 Multiple Indicator Cluster Survey (MICS) related to the reported health inequities, and explores potential policy recommendations and stakeholder responsibilities for mitigating these disparities.
Methods
Study design and participants
Qualitative descriptive design with in-depth interviews was used. Purposeful sampling approach was applied to select participants who can provide in-depth insights related to health disparities in Palestine. Participants were chosen from different backgrounds to capture a wider range of perspectives. Participants were chosen for their experience and good knowledge in the Palestinian health sector, and with senior position that is related to the subject being studied. MoH participants include senior representatives from different relevant units or departments inside the ministry. Interviews were only conducted with participants who were willing, available, and consented to be interviewed.
Interviews were conducted until saturation was reached, verbatim transcripts and initial coding were written immediately after each interview to highlight the major insights of each participant. Once researchers realized that no new codes or insights were emerging, then saturation was likely reached. A total of sixteen interviewees participated in this study and presented different perspectives about health disparities in Palestine. Seven participants were from MoH senior staff, two from the World Health Organization country office (WHO), three from other representative UN agencies (UNRWA, UNICEF and UNFPA), one representative of the private health sector, and three representing the NGOs sector (Palestinian Medical Relief Society (PMRS) and Palestinian Red Crescent Society (PRCS)). The sample included 6 females and 10 males from different geographical localities in the West Bank and Gaza Strip (Table 1).
Study tool
Semi-structured in-depth interviews were conducted with the selected respondents. An interview guide is prepared including main questions, follow-up and proping questions. The guide included questions about the aspects or areas of healthcare disparities within the Palestinian context, underlying contributing factors for these disparities, aspects of health inequities found in the most recent Multiple Indicators Cluster Survey conducted in 2019 (MICS 2019), current and recommended policies to tackle health inequities, roles and responsibilities of different stakeholders. The interview guide was reviewed by three independent public health experts from World Health Organization, PMoH and academia [17]. The interview guide was also pretested through two preliminary interviews to confirm its credibility and consistency.
Ethical approval for this study was obtained from the Research Ethics Committee et al.-Quds University. Participation in these interviews was voluntary, participants were asked to sign a specially designed consent form before conducting the interview. Participants were reassured of the confidentiality and anonymity of their participation.
Data collection
Eight interviews were arranged face-to-face, and another eight interviews were carried out virtually, all interviews were audio recorded. The average interview duration is about 45 min. The interviews were conducted by the first author during the months of September to October 2023. To enhance participants’ comfort and ability to express themselves, the interviews were conducted in the language preferred by the participant (either English or Arabic).
Data analysis
Qualitative content analysis for each interview was conducted manually to analyze data in accordance with the steps outlined by Graneheim and Lundman [18], It is a flexible data analysis method that deals with the manifest content of texts and the interpretation of the latent texts’ content. Themes raised from the analysis represent the latent meaning, while subthemes represent the manifest meaning in the same way as categories do according to Graneheim and Lundman’s analysis framework.
Verbatim transcripts were produced for each interview. The transcripts were reviewed several times to gain a comprehensive sense of the whole participants’ perceptions and thoughts, followed by deep analysis. The interviews were divided into meaning units of sentences, or paragraphs. These meaning units were then condensed into shorter statements, abstracted, and labeled with a code. Finally, through reflective and collaborative discussions among the authors, the codes were grouped into subthemes and themes. To enhance conformability and trustworthiness, and to decrease personal bias, the authors analyzed the transcripts individually and then discussed the analysis together until agreement was reached to ensure the proper selection of the meaning units, codes, subthemes, and themes.
Findings: results
Three main themes and eleven subthemes were extracted and realized through content analysis as summarized in Table 2. The three themes are: areas of health disparities, factors contributing to health disparities, and policy recommendations to enhance health equity. While Table 3 includes illustrative quotes for each subtheme (at the end of the article).
Theme one: areas of health disparities
All participants agreed that health disparities are noticed in the Palestinian health system in different areas and from different aspects. This theme highlights the specific domains where health disparities exist. Three subthemes are recognized as main areas of health disparities: disparities in healthcare services provision, disparities in healthcare coverage and disparities in healthcare outcomes.
Subtheme 1.1: healthcare services provision
This subtheme represents the domains of health disparities related to service provision as raised by participants. These include disparities in primary healthcare services availability and accessibility, disparities in hospital services provision, distribution, and quality of care. Preferences for service expansion and hospital care provision in larger governorates and urban areas are seen compared to smaller governorates and rural areas. Disparities in the quality of care have also been raised from different dimensions, including staff availability and patient contact time, workload, working hours, and waiting time.
“There are clear differences in the provision of healthcare services which also affect the quality of services. We clearly notice that the process of development and expansion in infrastructure is concentrated in specific areas, for instance, much more in cities than in villages and remote areas. It is also concentrated in the main large governorates compared to much less development in the smaller governorates. There is also a disparity in the workload between different clinics and primary healthcare centers. In some centers, a doctor treats 100 patients every day, which prevents the doctor from giving each patient the care they deserve.” (Participant 4, Female).
Most participants talked about the discrepancies of service provision between the West Bank and the Gaza Strip from different aspects. They raised the differences in the provision of medications and treatments explaining that Gaza Strip is facing inadequate provision of some expensive medications or treatments, and lack of some services like radiology services.
"The governmental sector in Gaza Strip faces chronic shortages of essential drug and supplies with a deficit reaching 40–50% consistently. We have to be realistic and admit that the Ministry of Health's warehouses are not stocked in the same way in all localities. People in major cities tend to have better services compared to those in peripheral areas." (Participant 12, Male).
Subtheme 1.2: health outcomes
This subtheme represents the disparities in health indicators and health status among different community groups or different Palestinian geographical areas. The main area of health outcomes emphasized by participants was the disparities in indicators related to reproductive health and child health indicators as seen in (MICS 2019) which revealed noticeable discrepancies in many health indicators between different geographical localities and different income quantiles, disparities were highly noticeable in indicators related to adolescents’ fertility rates, infant mortality rates, antenatal care and post-natal care. Most of interviewees emphasized that such disparities are mostly related to cultural and socioeconomic factors.
“The MICS results certainly indicate differences in health indicators, both at the level of the West Bank and Gaza, also at the governorates level in the West Bank. We need to consider subgroup analysis for different health indicators, for example the maternal mortality in Gaza Strip reached more than 60, while at the national level it is less than that and was 47. There are many health problems that are found in rural or remote areas, area C, and areas that have inadequate service provision.” (Participant 13, Male).
Subtheme 1.3: health coverage
This subtheme presents discrepancies and issues related to health insurance as raised by the interviewees, including disparities between the governmental health insurance scheme and UNRWA health insurance scheme, disparities between public insurance and private insurance, and disparities within the subcategories of the governmental insurance scheme itself.
"UNRWA clinics are proverbial… but they only serve the refugees. UNRWA insurance doesn’t cover everything…it provides extensive and free coverage for primary healthcare with high quality services. UNRWA hospital coverage requires significant copayments.” (Participant 13, Male).
Participants also raised the differences in health coverage among various groups covered by governmental health insurance such as public sector employees, low-income families, the unemployed, and workers. They highlighted the disparities in referral coverage, premiums and copayments between these different subgroups within the governmental health insurance system. “There are disparities within the governmental insurance system related to referral coverage based on subtype of insurance. The percentage of coverage varies and ranges between 70–100% depending on type of services and type of insurance” (Participant 2, Male).
Theme two: factors contributing to healthcare disparities
This theme presents the main underlying factors that contribute to health inequities within the Palestinian health context. Three subthemes are identified as main causing or contributing factors that are: Political related factors, socioeconomic and cultural related factors, and health system related factors.
Subtheme 2.1: political factors
All participants asserted that political situation resulting from the ongoing Israeli occupation has a major and direct negative impact on healthcare accessibility in different dimensions, Israeli occupation restrictions on patients’ movements through checkpoints and closures cause unequal access to health services, Israeli occupation policies of dividing Palestinian territories into three areas with different movement restriction for each area, Israeli occupation has the full authority in what is known as Area “C” of the West Bank including any developmental plans or building any new health facility or even expanding the existing ones need Israeli permission. Israeli occupation is controlling and devastating every Palestinian attempt for development.
“Israeli occupation is the main concern and the root causing factor in healthcare access inequity. Occupation controls everything. It prevents development and expansion of services in Jerusalem and area C, destroys new clinics in area C. Occupation is considered the major obstacle for implementing our developmental plans. Israeli occupation is the main root cause for outcomes disparities, due to its policies of closure, and checkpoints.” (Participant 5, Male)
Another point raised by many participants is the link between vulnerability or vulnerable groups and Israeli occupation. High rates of poverty and unemployment attributed to the Israeli occupation have contributed to increased vulnerability within the Palestinian community. Participants confirmed that disparities in healthcare accessibility are highly noticeable among vulnerable areas highly affected by Israeli soldiers’ or settlers’ violations such as certain localities in Jerusalem and Hebron governorates.
“Mapping vulnerabilities and vulnerable areas reveals links between health outcomes and vulnerability caused by aggressive occupation policies in areas like H2 in Hebron, seam zone, area C. The situation in East Jerusalem suburbs is complex due to poor living conditions and complicated special political situation.” (Participant 3, Male)
Subtheme 2.2: health system factors
This subtheme highlights several internal factors and limitations within the Palestinian health system that contribute directly or indirectly to health disparities. The main issue raised by most participants is the shortages in human resources and financial resources, that is highly affecting the provision of adequate services equally in different locations. The current governmental financial crisis has further contributed to resources deficiency.
“The main causing factors for disparities are inadequate human resources and inadequate budget for running costs. Lack of adequate budget negatively affects the availability of human resources, equipment, lab materials, to provide health services”.(Participant 5, Male)
Participants also raised the issue of inadequate policies and interventions to minimize health inequalities, improper and unequal implementation of policies and regulations, like the implementation of universal free coverage for children under six years old as stated in the Palestinian Law.
"Although the the National Palestinian Basic Law has stated free coverage for children under six years old, implementation varries between WB and GS. There is no clear implementation approch, leading to disparities in policy and regulation implementation between WB and GS, including health coverage for children. Also, disparities between MOH and UNRWA creates differences in obtaining service. It is unclear who is responsible for implementing these policies, and some policies are poorly implemented due to the lack of resources (example nutritional supplementation)".(Participant 4, Female)
Participants also asserted that lack of health research and disaggregated data in many healthcare indicators negatively affects the monitoring of inequalities within the Palestinian health system.
"There is no measuring or monitoring of inequities among the Palestinian population including different vulnerable groups. We don’t have adequate evidence or research that would guide you to who are the marginalized groups and what would be the right tools to address them”. (Participant 6, Female)
Subtheme 2.3: socioeconomic-cultural factors
This subtheme presents several issues related to the Palestinian culture and values that affect healthcare accessibility including gender-related values, women liberty, and tribal rule in some areas. Cultural differences between urban and rural communities have direct impact on healthcare accessibility disparities. The prominent conservative cultural believes in the Palestinian community about women free movement are highly affecting women access to healthcare services.
”Health disparities are affected by health access behavior which differs between city and village. In rural areas, woman can’t go alone to the clinic, husband or mother-in-law should accompany the wife. Health access behavior is determined by cultural and social aspects, personal attitude, knowledge and practices, social and economic status, and attitudes of healthcare workers. Further analysis of these barriers is needed”. (Participant 9, Female)
Participants also raised different social factors and argued its impact on healthcare disparities including, level of education, poverty and income, place of residency, disability status. awareness and health knowledge.
“Health awareness plays a major role in health equity; community awareness affects their health access and thus determines health outcomes or status. We in Palestine believe that we should visit the doctor only when getting sick or feel pain, but we lack awareness for preventive care and routine checkup. Rural and Bedouin communities are busy in their land work; they are usually less educated and lower level of awareness”. (Participant 5, Male)
Theme three: policy recommendations to enhance healthcare equity
This theme presents a set of policy recommendations raised by participants to minimize or target health disparities and promote better health equity in Palestine. Participants proposed five main subthemes as policy recommendations to promote healthcare equity in Palestine that are: Integrating health equity into different policy frameworks, Strengthening MoH leadership and collaborative partnerships to advance health equity, Enhancing healthcare infrastructure and delivery approach, Reforming the health insurance system for better equity and efficiency and universal coverage, and Fostering community awareness and advocacy for advancing health equity and the right to health for all Palestinian.
Subtheme 3.1: integrating health equity into different policy frameworks
Participants agreed that healthcare equity should be prioritized and integrated within all policies and policy making processes. Precise policies that target healthcare equity are needed through targeting the underlying contributing factors and social determinants of health, enhanced monitoring for the Palestinian health system performance and health disparities through better disaggregated data, strengthening strategic planning process that is based on deep situation analysis and evidence-based policy making, strengthening plans implementation process and promote equity in resource allocation. All participants asserted that health equity should be targeted within national policies in a more specific and effective manner,
“We need real actionable direct policies targeting the roots and causes of inequity. Without a clear policy with a specific goal and specific interventions, we will not achieve the goal of improving quality of health services and equity for all Palestinians”. (Participant 1, Male)
Some participants confirmed the need for realistic and thorough analysis for health disparities, with a focus on implementing of plans that specifically target the inequality and monitoring relevant indicators.
"There is a need for a deeper understanding of health disparities, and how they are being addressed. You need to have a clear evidence-based plan at the policy level to effectively reduce these disparities.” (Participant 6, Female)
Subtheme 3.2: strengthening MoH leadership and fostering collaborative partnerships to advance health equity
This subtheme is mainly related to the roles of the different actors. which should be well- coordinated and led by the MoH as the primary governmental authority. Participants emphasized the importance of leadership and political will in prioritizing health equity.
“There is a need to strengthen the Ministry of Health stewardship role in eliminating disparities including the monitoring role and encouraging inter-sectoral collaboration between different service provider and all partners to work comprehensively in tackling inequalities.” (Participant 6, Female)
Also, all participants emphasized the necessary cooperative and coordinated roles of all stakeholders to minimize health disparities. They explained about the cooperative roles in service provision, targeting vulnerable groups, monitoring health system performance and disparities, participatory policymaking, advocacy and resources mobilization, community awareness and health education, targeting social determinants of health.
Subtheme 3.3: enhancing healthcare infrastructure and delivery approach
Participants also emphasized the need to enhance healthcare structure and delivery approach to achieve better equity and bridge gaps in service provision and resources allocation. They highlighted several successful and recommended approaches to expand access in marginalized communities including mobile clinics for Bedouin communities, extending working hours in villages, strengthening primary healthcare provision through a family practice approach, expanding hospital services to localize services and achieving universal health coverage.
“Ministry of Health pays great attention to mobile clinics to reach all marginalized groups. We have accordingly expanded mobile clinics in cooperation with our partners. We are also working to provide ambulances and emergency centers in these remote areas. Family health approach will contribute to improve access to PHC services and ensure its provision for all. We are establishing our own services and working to guarantee the basic rights to health for all citizens."(Participant 9, Female)
Subtheme 3.4: reforming the health insurance system for better equity and efficiency and universal coverage
This subtheme emphasized the need to improve and reform the health insurance system to ensure equitable coverage and better efficiency. Participants raised several suggestions including comprehensive insurance system, compulsory health insurance, universal coverage of vulnerable groups, and specific coverage for women, children and victims of gender-based violence. Other recommendations included unified coverage for all groups, establishing national health insurance, updating the basket of services, and reviewing the premium and copayment systems. Regardless of the specific proposed suggestions, all participants on the necessity to review and reform the current health insurance.
"Looking at the issue of health insurance; everyone calls for the necessity of reviewing health insurance... and working to establish a comprehensive health insurance to cover all people and achieve equity. Each citizen should be covered by health insurance". (Participant 12, Male)
Subtheme 3.5: fostering community awareness and advocacy for advancing health equity and the right to health for all
This subtheme highlights the necessity of promoting community awareness and advocacy for health equity and right to health for all Palestinians. Many participants stressed the role of community participation in promoting healthcare equity through social networking, and participatory role in decision making, social advocacy for vulnerable groups’ needs (Fig. 1).

Summary of the main study finding’s themes and subthemes
“We need to enhance the role of community in health education and awareness. This can be achieved by involving local figures, such as women from the same village or religious leaders participate in the community awareness efforts”. (Participant 9, Female)
Participants stressed that advocacy for equal health rights should be strengthened and managed by various actors including the government and the Ministry of Health, the non-governmental organizations, and the international organizations such as the World Health Organization and other United Nations organizations.
"We advocate for the “right to health” for every citizen, a principle upheld by various conventions and international agreements. Our recommendation is keeping health issues separate from politics. We urge all partners to exert greater pressure on the occupation”. (Participant 8, Male)
Such complementary role between different actors has been assured by participants from different aspects. In addition to their role in advocacy and community awareness, participants also recommended the necessity of complementary role in service provision, leading role for MoH in policymaking with the participatory approach for all stakeholders.
Discussion
In view of the paucity of published papers on perspectives of key stakeholders regarding health disparities in Palestine, the current study extends current knowledge about health disparities in the Palestinian health system. The different stakeholders’ perspectives revealed in this study are aligned with evidence seen in literature concerning the presence of health disparities in Palestine in different aspects, that are mostly associated with the complex context of the Palestinian health system and barriers imposed by the Israeli occupation. Overall, the results show the inadequate awareness and concern of stakeholders on health equity, lack of proper policies addressing health equity and social determinants of health in Palestine on the ground.
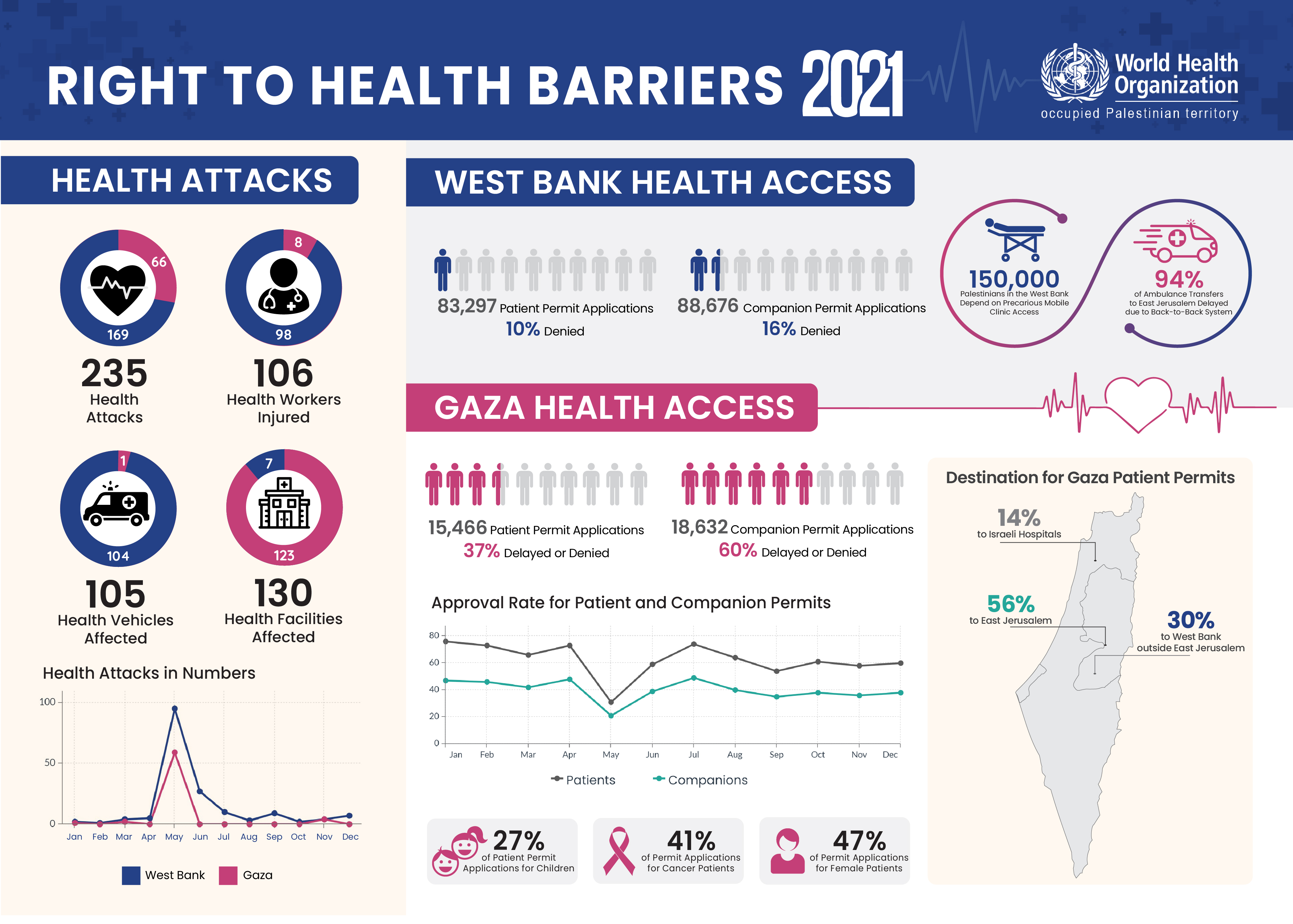
Disparities in healthcare provision and accessibility have been primarily viewed on many occasions as health access barriers caused mainly by Israeli occupation restrictions, especially among vulnerable communities. Disparities in health access between West Bank and Gaza Strip have been verified in WHO periodic reports for monitoring health access in Palestine. The WHO country office of Palestine monitors health access for Palestinian patients and produces periodic reports indicating the number of patients referred for medical treatment in East Jerusalem hospitals or Israeli hospitals who routinely require Israeli permission. In 2021, 37% of permit applications from Gaza Strip patients were denied or delayed, compared to 10% of West Bank patients [19].
Disparities in health services provision have been also cited in the National Health Strategy 2021–2023, indicating the presence of noticeable differences in the number of hospital beds or PHC centers among different governorates, in addition to noticeable differences in workload on the facility and governorate levels [20].
Disparities in health coverage are verified by the fact that several health insurance schemes are used in Palestine with different eligibility criteria and different benefit package. Health insurance schemes include the government health insurance (GHI) scheme, the UNRWA health insurance scheme and the private health insurance. The GHI is managed and regulated under the responsibility of the PMoH where enrollment procedures, eligibility regulations, coverage and patients’ contribution rates are all determined through several subgrouping system that is related to enrollment type or supporting entity, subgroups include: voluntary enrolment for all citizens, obligatory enrolment for governmental employee, free enrollment for selected social subgroups such as hemophilia and thalassemia patients, labors subgroup through labors’ association, poor families covered through the Ministry of Social Development, and several other subgroups [12, 13].
The GHI covers its participants with all health services to fulfill their health needs ‘as possible’ through a comprehensive and inclusive benefits package of services. The UNRWA health insurance provides coverage for refugees only, without any premium prepayment for participation. UNRWA scheme provides free primary health care through the UNRWA healthcare centers and purchases secondary and tertiary care from other providers, but with high copayment rate reaching 30% of total referral cost [13].
Inequalities in health outcomes in Palestine have been linked to disparities in socioeconomic determinants of health; however, the absence of data that is socially and geographically disaggregated is considered a significant challenge for deeper analysis [5]. The most available evidence for disaggregated data is the Multiple Indicators Cluster Survey (MICS) carried out every five years; the 2019 MICS indicates noticeable disparities in reproductive health outcomes among different social groups, such discrepancies in relevant indicators are clearly linked with socioeconomic factors such as geographical location in rural areas, income quantile, mother age and education. Post-neonatal mortality rate in camps is found to be 7.0 compared to 3.4 in rural and 2.2 in urban areas, the adolescents birth rate in Gaza Strip is 48 compared to 39 in West Bank, and it is also 72 in the poorest quantile compared to 21 in the richest quantile [4]. The intersection between health disparities and social determinants of health has been widely discussed in literature [21,22,23]. The WHO Commission on Social Determinants of Health (CSDH) has developed a comprehensive framework to address growing health inequities through tackling its root causes of the Social Determinants of Health (SDH) [23].
Health has always been linked to politics worldwide, but in the Palestinian context politics is probably considered the major determinant for health, with strong recognition that political forces are controlling Palestinians lives and health through the longstanding Israeli occupation and Zionist settler colonialism causing geographical and health fragmentations [24]. The impact of political and armed conflict on health disparities has been stated in literature from several aspects and through several examples from different conflict areas all over the world. Political or armed conflict has contributed to the fragility of the health system in the affected areas through direct health infrastructure destruction, supply chain disruption, health delivery systems disturbances and fleeing health personnel, in addition to its circumstantial impact on the water and food supply and loss of shelters. Furthermore, those who have endured considerable loss as a result of the conflict are found to be more vulnerable to ill-health and ill-being [25, 26].
Exposure to longstanding armed or political conflict usually also leads to displacement and impoverishment, psychological trauma, malnutrition, increased rates of infectious diseases and illnesses. It is worth noting that the occupied Palestinian territory is living in chronic political and armed conflict since 1967. This conflict has resulted in several intensified fluctuations that have caused disruptions and disparities in healthcare access, destroyed infrastructural through direct attacks on health facilities and personnel, geographical fragmentation and deteriorating socioeconomic conditions. The health system is currently facing catastrophic crisis after October 7th conflict in Gaza Strip, the majority of healthcare facilities are out of service and those hospitals that are still operating are only partially functional and lacking basic medicines and supplies to treat patients [27,28,29].
It is evident that politics and the ongoing Israeli occupation have led to health and social disparities within the Palestinian community; the situation has become worse due to the geographical and political fragmentation between West Bank and Gaza Strip. Such fragmentation and its impact on health disparities was clearly manifested during COVID-19 pandemic crisis, where the disparities in health resources and the division in health systems’ decisions and policy disparities were very clear. While early preventative lockdown measures were effectively taken in the West Bank, the response was slow in Gaza Strip [30].
In the same aspect, the political situation and Israeli occupation are significantly affecting health access in Palestine; occupation-imposed transportation limitations are consistently correlated with a decline in health outcomes and healthcare access [31]. Nasr et al. study has analyzed healthcare disparities based on the PCBS data of the 2018 Social and Economic Living Conditions Survey (SEFSEC), the study found that clear disparities exist both in terms of health status and health access, and these disparities are mainly associated with geographic location and socioeconomic conditions that are further exacerbated in the Gaza Strip [32]. Nasr et al. study has also confirmed that poorer and less educated people fare worse both in terms of health access as well as in health status, in addition to the clear disparities between the West Bank and Gaza Strip in terms of health access and status indicators, and clear disparities in terms of health access between those living in area C compared to those living in non-area C in the West Bank [32].
Similar findings are found in different conflict-affected areas, where disparities in access to primary healthcare services were noticed during and after the conflict and linked to the conflict intensity and associated socioeconomic impact [33,34,35]. One study comparing healthcare access in four different conflict-affected countries found that PHC access varied across subnational regions in the four studied countries; more prevalent financial than geographic barriers to care, the magnitude of both educational and wealth disparities in access to care was higher with geographic proximity to medium or high intensity conflict. It was noted that a higher magnitude of disparity was observed in neighborhoods surrounded by medium or high-intensity conflict compared to no or low intensity conflict, and higher magnitude of wealth rather than educational disparities was also likely to be observed in the four studied contexts [35].
Several research papers have indicated that diverse range of factors playing role in determining health outcomes within the Palestinian community including socioeconomic, demographic, and cultural factors. Evidence is taken from studies analyzing disparities in the status of women health, mental health, child health and nutrition [36,37,38,39,40]. Geographic and residential factors, together with socioeconomic status, are evident key factors to understanding differences between women’s self-reported health status in Palestine [38]. Studies have also asserted that poor awareness of healthy diets, poverty, poor socioeconomic situations, urbanization, community lifestyle, political situation and the blockade are the major determinants for disparities in the nutritional status of Palestinian children [31, 40,41,42].
The relationship between health disparities and social determinants of health has been raised by policymakers in different settings and several similar studies. Henson and her colleagues explored the senior American health officer’s conceptualization about health disparities; the participants in their study confirmed that health disparities are rooted in social and economic determinants of health, and health equity achievement needs redistributions of opportunities or resources [43]. Another study aimed to understand of the development and implementation of health equity indicators in Iran through exploring the perspective of policy makers and executive officers. The study's findings categorized the concept of health equity into two areas: equity in health outcomes and equity in healthcare system that is associated with fair distribution of services, access to and possibility of benefiting from health services [44].
Participants’ recommendations to promote health equity reflect their believes for the need for stronger policymaking process in the Palestinian health system. This includes different stages of the policymaking process that are situational analysis for health disparities, policy formulation aiming to prioritize and specifically target health equity, enhancing policy implementation through proper and adequate resources allocation, coordinated efforts and roles for all stakeholders, implementing comprehensive reform processes in service delivery approach and healthcare coverage, strengthening monitoring and evaluation processes. The call for health reform in the Palestinian health system is not new [45], Catastrophic out-of-pocket healthcare payment is considered high in Palestine and calls for health insurance reform have been stated on several occasions [12, 46,47,48].
Multidimensional and well-coordinated efforts are needed to tackle health disparities within the complicated Palestinian context. A comprehensive health system strengthening approach could be beneficial to mitigate vulnerabilities and promote health equity, through targeting the different pillars of health system strengthening efficiently and effectively. Priority interventions should include good governance and policy reform in different aspects including health financing and health insurance, improving access to healthcare services through more efficient and effective healthcare delivery model, addressing social determinants of health, cross-sectoral and intersectoral coordination including effective community participation and health awareness.
Study limitations
The healthcare providers are broad and numerous, including the Ministry of Health (MoH), UNRWA, NGOs, and private organizations in both the West Bank and Gaza Strip. Therefore, we ensured that the perspectives of stakeholders were captured by having a purposive sample that included participants from different backgrounds to ensure diversity of perspectives.
While our study is among the few that explore the perspectives of policymakers and various health stakeholders regarding health disparities within the Palestinian healthcare system, we did not include intersectoral actors' perspectives. Future research may focus on exploring these perspectives to gain more insights in this area.
Implications for future research
The findings of this study highlight several areas to be investigated in future research. Future research should focus on gathering data that is broken down by social, geographic, and demographic factors to better understand the disparities and specific needs of different population groups. In the same context, future research could deeply investigate the impact of different relevant factors on health equity including the impact of occupation and conflict on health equity, the impact of the current social policies and health policies on health equity. Also analyzing the equity dimension in the different health system building blocks, identifying and evaluating successful health interventions and best practices to promote health equity.
Implications for policymaking process
The findings of this study argue policymakers to drive evidence-based policy making and comprehensive reforms in the Palestinian healthcare system to improve equity in healthcare access and coverage. The study highlights the need for equity-focused policies aimed at reducing health disparities, and the need for preventive measures designed to address root causing factors including the social determinants of health.
The recommended policy interventions from the participants illustrate the consensus for specific and efficient policies targeting equitable coverage through health insurance reform, and equitable access through reforming healthcare delivery structure. It also highlights the importance of multisectoral and stakeholders’ collaboration, and community engagement in the development and implementation of health interventions.
Conclusion
Our study explored health disparities in Palestine from the perspectives of policymakers and key stakeholders across various health sectors. The study identified health inequities, areas of disparities and contributing factors providing a policy spotlight for improving health equity in Palestine.
Promoting evidence-based policymaking and fostering a shared responsibility among all stakeholders are essential for the success of health equity initiatives. Prioritizing health equity will lead to sustainable improvements in public health, economic and social gains, and improved health outcomes.
Data availability
No datasets were generated or analysed during the current study.
References
Braveman P, Gruskin S. Defining equity in health. J Epidemiol Community Health (1978). 2003;57(4):254–8.
Whitehead M, Dahlgren G. Concepts and principles for tackling social inequities in health: levelling up part 1. World Health Organization: Studies on social and economic determinants of population health. 2006;2:460–74.
Braveman PA, Kumanyika S, Fielding J, LaVeist T, Borrell LN, Manderscheid R, et al. Health disparities and health equity: the issue is justice. Am J Public Health. 2011;101(S1):S149–55.
Palestinian Central Bureau of Statistics. Palestinian Multiple Indicator Cluster Survey 2019-2020, Survey Findings Report. Ramallah: Palestinian Central Bureau of Statistics; 2021.
Fahoum K, Abuelaish I. Occupation, settlement, and the social determinants of health for West Bank Palestinians. Med Confl Surviv. 2019;35(3):265–83.
Waterston T, Nasser D. Access to healthcare for children in Palestine. BMJ Paediatr Open. 2017;1(1):e000115. https://doiorg.publicaciones.saludcastillayleon.es/10.1136/bmjpo-2017-000115.
Vitullo A, Soboh A, Oskarsson J, Atatrah T, Lafi M, Laurance T. Barriers to the access to health services in the occupied Palestinian territory: a cohort study. The Lancet. 2012;380:S18–9.
UN Economic, Social Council. Economic and social repercussions of the israeli occupation on the living conditions of the Palestinian people in the occupied Palestinian territory, including East Jerusalem, and of the Arab population in the occupied Syrian Golan. Note by the Secretary-General A/73/87–E/2018/69 New York. 2018.
Palestinian Central Bureau of Statistics (PCBS). Unleashing the power of gender equality: Uplifting the voices of women and girls to unlock our world’s infinite possibilities. Ramallah: PCBS; 2023. Available from: https://www.pcbs.gov.ps/post.aspx?lang=en&ItemID=4544.
World Bank. Racing Against Time: World Bank Economic Monitoring Report to the Ad Hoc Liaison Committee. Washington: DC; 2023S.
PCBS. Statistical yearbook of Palestine, 2022. Ramallah; 2022. Available from: https://www.pcbs.gov.ps/Downloads/book2637.pdf. Cited 2024 Oct 25.
Abu-Mughli F. Coalition for Accountability and Integrity (AMAN). Towards a comprehensive health insurance system. 2018.
Morrar R, Jabr S, Ghandour R, Abu-Rmeileh NME, Forgione DA, Younis M. Identifying healthcare cost drivers in Palestine. Int J Health Plann Manage. 2021;36(3):911–24.
Ministry of Health. National Health Strategy 2017-2022. Ramallah: Ministry of Health; 2017.
Collier J, Kienzler H. Barriers to cardiovascular disease secondary prevention care in the West Bank, Palestine–a health professional perspective. Confl Health. 2018;12:1–13.
Takruri A, Radwan M, El Jabari C, Nawajah I, Hassan S. Experiences of Palestinian patients with hospital services: a mixed-methods study. BMJ Open Qual. 2023;12(2): e002118.
Roberts RE. Qualitative interview questions: guidance for novice researchers. Qual Rep. 2020;25(9):3185.
Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–12.
World Health Organization. Occupied Palestinian Territory. 2022. Right to health barriers: 2021. Available from: http://www.emro.who.int/images/stories/palestine/right-to-health-barriers-2021.jpg?ua=1. Cited 2022 May 19.
Palestinian Ministry of Health. National Health Strategy 2021–2023. Ramallah: Ministry of Health; 2021.
Penman-Aguilar A, Talih M, Huang D, Moonesinghe R, Bouye K, Beckles G. Measurement of health disparities, health inequities, and social determinants of health to support the advancement of health equity. J Public Health Manag Pract. 2016;22:S33–42.
Schillinger D. The intersections between social determinants of health, health literacy, and health disparities. In: Logan R, Siegel E, editors. Health literacy in clinical practice and public health. Amsterdam: IOS Press; 2020. p. 22–41.
WHO. A conceptual framework for action on the social determinants of health. 2010. Available from: https://apps.who.int/iris/bitstream/handle/10665/44489/?sequence=1. Cited 2022 May 12.
Asi YM, Hammoudeh W, Mills D, Tanous O, Wispelwey B. Reassembling the pieces: Settler colonialism and the reconception of Palestinian health. Health Hum Rights. 2022;24(2):229.
Sinha S, Liang J, Sinha S, Liang J. Deep vulnerabilities and coping after conflict: Ill-health, treatment seeking behaviour and informal medical practices in the borderland. In: Health inequities in conflict-affected areas: armed violence, survival and post-conflict recovery in the Indo-Bhutan borderlands. 2021. p. 181–223.
Sinha S, Liang J, Sinha S, Liang J. Armed violence and the breakdown of the health system: vulnerabilities of health personnel in the conflict-affected borderland. Health inequities in conflict-affected areas: armed violence, survival and post-conflict recovery in the Indo-Bhutan borderlands. 2021:113–41.
Beiraghdar F, Momeni J, Hosseini E, Panahi Y, Negah SS. Health crisis in Gaza: The urgent need for international action. Iran J Public Health. 2023;52(12):2478.
London L, Watterson A, Mergler D, Albin M, Andrade-Rivas F, Di CA, et al. A call from 40 public health scientists for an end to the continuing humanitarian and environmental catastrophe in Gaza. Environ Health. 2024;23(1):59.
Parker C, Sly L, Balousha H, Ayyoub L. Gaza hospital evacuated as Israel intensifies campaign in the north. The Washington Post. 2023. Available from: https://go.gale.com/ps/i.do?id=GALE%7CA773294135&sid=googleScholar&v=2.1&it=r&linkaccess=abs&issn=01908286&p=AONE&sw=w&userGroupName=anon%7Ea8a13412&aty=openweb-entry.
AlKhaldi M, Kaloti R, Shella D, Al Basuoni A, Meghari H. Health system’s response to the COVID-19 pandemic in conflict settings: Policy reflections from Palestine. Glob Public Health. 2020;15(8):1244–56.
Jabali O, Ayyoub AA, Jabali S. Navigating health challenges: the interplay between occupation-imposed movement restrictions, healthcare access, and community resilience. BMC Public Health. 2024;24(1):1297.
Nasr S, Mitwalli S, Hammoudeh W. Examining Health Inequalities in the occupied Palestinian territory. Birzeit: Institute of Community and Public Health; 2021.
Omam LA, Jarman E, O’Laughlin KN, Parkes-Ratanshi R. Primary healthcare delivery models in African conflict-affected settings: a systematic review. Confl Health. 2023;17(1):34.
Ramadan M, Tappis H, Brieger W. Primary healthcare quality in conflict and fragility: a subnational analysis of disparities using population health surveys. Confl Health. 2022;16(1):36.
Ramadan M, Tappis H, Uribe MV, Brieger W. Access to primary healthcare services in conflict-affected fragile states: a subnational descriptive analysis of educational and wealth disparities in Cameroon, Democratic Republic of Congo, Mali, and Nigeria. Int J Equity Health. 2021;20(1):253.
Hammoudeh W, Mitwalli S, Kafri R, Lin TK, Giacaman R, Leone T. The mental health impact of multiple deprivations under protracted conflict: A multi-level study in the occupied Palestinian territory. PLOS global public health. 2022;2(12): e0001239.
Giacaman R, Leone T, Alburez-Gutierrez D, Ghandour R, Coast E. Maternal and child access to care and intensity of conflict in the occupied Palestinian territory: a pseudo-longitudinal analysis (2000–2014). 2019.
Bates K, Leone T, Ghandour R, Mitwalli S, Nasr S, Coast E, et al. Women’s health in the occupied Palestinian territories: contextual influences on subjective and objective health measures. PLoS ONE. 2017;12(10): e0186610.
Massad S, Deckelbaum RJ, Gebre-Medhin M, Holleran S, Dary O, Obeidi M, et al. Double burden of undernutrition and obesity in Palestinian schoolchildren: a cross-sectional study. Food Nutr Bull. 2016;37(2):144–52.
Massad S, Gebre-Medhin M, Dary O, Abdalla M, Holleran S, Karmally W, et al. Micronutrient status of Palestinian school children following salt and flour fortification: a cross-sectional study. BMC Nutr. 2020;6(1):38. https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s40795-020-00367-2.
A. Assaf E, Al Sabbah H, Al-Jawadleh A. Analysis of the nutritional status in the Palestinian territory: a review study. Front Nutr. 2023;10:1206090.
Al-Lahham S, Jaradat N, Altamimi M, Anabtawi O, Irshid A, AlQub M, et al. Prevalence of underweight, overweight and obesity among Palestinian school-age children and the associated risk factors: a cross sectional study. BMC Pediatr. 2019;19:1–13.
Henson RM, Mcginty M, Juliano C, Purtle J. Big City health officials’ conceptualizations of health equity. J Public Health Manag Pract. 2019;25(4):332–41.
Ravaghi H, Goshtaei M, Manesh AO, Abolhassani N, Arabloo J. Stakeholders’ perspective on health equity and its indicators in Iran: a qualitative study. Med J Islam Repub Iran. 2015;29:250.
Mataria A, Khatib R, Donaldson C, Bossert T, Hunter DJ, Alsayed F, et al. The health-care system: an assessment and reform agenda. The Lancet. 2009;373(9670):1207–17.
Mataria A, Raad F, Abu-Zaineh M, Donaldson C. Catastrophic healthcare payments and impoverishment in the occupied Palestinian territory. Appl Health Econ Health Policy. 2010;8:393–405.
Abu-Zaineh M, Mataria A, Luchini S, Moatti JP. Equity in health care finance in Palestine: the triple effects revealed. J Health Econ. 2009;28(6):1071–80.
Palestinian Ministry of Health. National health strategy 2017-2022. Ramallah; 2017.
Acknowledgements
The authors would thank people who participated in this study.
Funding
Authors declare that no funding was received for this study.
Author information
Authors and Affiliations
Contributions
O. A.: conceived the study, collected, and analyzed data, prepared the manuscript. A.I. analyzed the data and supervised the study's conception, design and collection. K. E. analyzed the data. All authors contributed significantly to the data analysis, agreed and approved the final analysis for the themes and subthemes. They all also agreed on the final revision of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was obtained from the Research Ethic Committee of Al-Quds University (REF number: 05/ 2023). In addition, before conducting key informant interviews, key informants provided written or verbally recorded informed consent.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

{kind=link}
Cite this article
Al Eker, O., Imam, A. & Elissa, K. Unveiling health disparities in Palestine: a qualitative study of stakeholders' perspectives. Int J Equity Health 24, 102 (2025). https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s12939-025-02449-8
Received:
Accepted:
Published:
DOI: https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s12939-025-02449-8